
Bij openhartoperaties in het Erasmus MC wordt het hart rondom bemeten met geavanceerde elektrodes uit Delft. Hoe verloopt die samenwerking op zoek naar hartritmestoornissen?
- In 2021 kwamen er negen Medical Delta-hoogleraren bij. Dat zijn professoren met een aanstelling aan een academisch ziekenhuis (LUMC of Erasmus MC) en aan de TU Delft. Dat bracht het totaal van MD-hoogleraren naar 22. Kennelijk een succesformule. Hoe werkt zo’n dubbelaanstelling in de praktijk? Dat is de achterliggende vraag in deze miniserie onderzoeksportretten.
Aan de elektrodes in de vitrinekast is de technische ontwikkeling van de laatste twintig jaar af te lezen. De oudste ziet eruit als een soort kleine douchekop waar vier kabels uitkomen die eindigen in aangeschroefde stekkers van het formaat computermuis. Die gebruikte Natasja de Groot bij haar promotieonderzoek in Leiden naar hartritmestoornissen. De nieuwste elektrode is een flinterdun stripje waaraan drie meter meerlaagse flatcable zit bevestigd om de 192 kanalen tegelijkertijd uit te lezen. Die kabel werd in Delft gemaakt in de groep bio-elektronica van prof.dr.ir. Wouter Serdijn (faculteit Elektrotechniek, Wiskunde en Informatica).
Een dag niet gedanst is een dag niet geleefd, vindt cardioloog-elektrofysioloog prof.dr. Natasja de Groot (Erasmus MC). In een vorig leven volgde ze een opleiding tot klassiek balletdanseres aan de balletacademie in Amsterdam. Maar toen blessures na tien jaar haar droomcarrière dwarsboomden, besloot ze naar het atheneum te gaan. Bij de biologielessen werd ze zodanig gegrepen door de werking van het hart dat ze besloot geneeskunde te gaan studeren in plaats van astronomie. Als kind wilde ze overdag danseres worden en ’s avonds astronaut. Het werd: cardioloog.
Tijdens haar medicijnenstudie ontwikkelde De Groot met haar gevoel voor patronen en ritmes een interesse in hartritmestoornissen – een wijdverbreide maar slecht begrepen aandoening. Een hart kan te snel slaan – tot wel 300 slagen per minuut – te langzaam, of zelfs een slag overslaan. “Meestal begint het met boezemfibrilleren, een paar seconden tot een paar minuten. Dan melden de meeste mensen zich met klachten bij de dokter”, aldus De Groot.
Dat kan iedereen overkomen, en de kans erop neemt toe met de leeftijd. Maar helaas is de interventie van ‘ablatie’ (beschadigen van hartweefsel om ongewenste geleiding te stoppen) maar matig effectief. Daarnaast zijn er onbegrepen methoden (zoals prikkelen van het oor) die hartritmestoornissen welswaar aanwijsbaar verminderen, maar waarvan het mechanisme niet bekend is. Er is kortom nog veel onduidelijk over hoe precies de levenspuls over en door het hart trekt. Vandaar dat De Groot zich de taak heeft gesteld om “de elektrische eigenschappen van het hart te kwantificeren.” Want daar begint alles mee.
Nieuwsgierig blijven
Ze doet dat sinds eind vorig jaar als Medical Delta-hoogleraar met een aanstelling aan zowel het Erasmus MC als aan de TU Delft. Ze heeft een onderzoeksteam met artsen, ingenieurs, een bioloog, een dierenarts, een klinisch technoloog en zelfs een astronoom. “Een leuk groepje vakidioten”, noemt ze haar team vertederd. “Iedereen heeft zijn eigen passie, maar ze vinden het ook allemaal leuk om bij een ander te kijken. Ze houden van wetenschap en ze blijven nieuwsgierig.” Ze beschrijft een cyclus waarin betere meetinstrumenten leiden tot betere metingen, betere analyses en betere vraagstellingen waarvoor weer betere instrumenten nodig zijn. “Zo houden we elkaar een beetje bezig.”

De elektrode met 192 contactpuntjes en de meerlaags platte kabel bij een modelhart op ware grootte. (Foto: Guus Schoonewille)
De meetcampagne begon in 2010. Ze kreeg toen hartchirurgen zover dat die bij iedere openhartoperatie op acht vastgestelde posities rondom het hart gedurende vijf seconden een speciale elektrode tegen het hart hielden voor de opname van de elektrische signalen. De laatste versie van de elektrode telt 192 contactpuntjes met onderlinge afstand van 2 millimeter. Dat zijn dus ruim 1.500 verschillende ECG’s per patiënt. Inmiddels zijn meer dan duizend patiënten zo bemeten en vormen ze samen een heel diverse groep. Sommigen hebben aangeboren hartfalen of hartritmestoornissen, anderen weer niet. Je kunt hooguit zeggen dat er bij iedereen wat aan het hart mankeerde. Uit de tienduizenden signalen heeft De Groot inmiddels wel de conclusie getrokken: “Elk hart is elektrisch uniek.”
“We rijden naar Delft”
Om betere grip te krijgen op al die data besloot ze dat ze de geleidingssnelheid wilde weten tussen meetpunten, want verschillen in de geleidingssnelheid bepalen hoe de stroompuls, die zoals wellicht bekend in de sinusknoop begint, zich over het hart verspreidt. Namelijk: via de weg van de minste weerstand. Ze nam contact op met collega-hoogleraar prof.dr.ir Ton van der Steen – natuurkundige en ultrasound-expert, en Medical Delta-hoogleraar van het eerste uur. Wist hij iemand die zulke berekeningen kon maken? Na een paar telefoontjes veerde hij op. “Kom op”, zei hij. “Trek je jas aan. We rijden naar Delft.”
Daar maakte ze kennis met prof.dr.ir. Alle-Jan van der Veen. Bij de afdeling micro-elektronica van de Elektrotechniek, Wiskunde en Informatica (EWI) had hij expertise opgebouwd over signaalbewerking voor communicatie en astronomie. Hoewel cardiologie heel wat anders is dan telecom, zijn de onderliggende wiskundige modellen vergelijkbaar: een signaal dat van A naar B loopt. Uit de ECG-signalen kon Van der Veen de geleidbaarheid ter plekke berekenen, een grootheid die onder meer de geleidingssnelheid bepaalt. De lokale geleidbaarheid van het hartweefsel wordt weergegeven in een kleurenkaart. Op sommige plekken treedt er een verstoring in de geleiding op die met zwarte blokjes wordt weergegeven. Dat kan duiden op littekenweefsel.
Al snel kwam prof.dr.ir. Wouter Serdijn (EWI) erbij voor verfijndere elektrodes. “Dat is geen rocket science”, zegt hij daar nu over. “Vaak kun je iemand uit een andere discipline al snel helpen met de bestaande stand van de techniek. Dat was toen een contactstripje en een meerlaags flexprint kabel voor de 192 signalen.”
Gezamenlijk onderzoek
In 2015 dienden de drie samen met een celbioloog prof.dr. Bianca Brundel uit Amsterdam UMC een onderzoeksaanvraag in bij CVON (Cardiovasculair Onderzoek Nederland, onderdeel van de Hartstichting) voor de opname en analyse van de bio-elektrische signalen van het hart. Dat is vooralsnog fundamenteel onderzoek naar de activatiepatronen van het hart. Wat is normaal en wat afwijkend?
Uiteindelijk moet het onderzoek leiden tot een beter meetinstrument voor diagnose om vast te stellen hoe ernstig de hartritmestoornissen zijn, en liefst ook naar een effectievere behandeling dan nu beschikbaar is.
Net als de elektronica de medische vraagstelling aanscherpt, gebeurt het omgekeerde ook. De drie meter flatcable is in praktijk best onhandig en de kabel pikt ook allerlei stoorsignalen op. Serdijn werkt er daarom samen met promovenda Sampi Rout aan een belangrijke verbetering van de aansluiting van de elektrode. Geen 192 draadjes meer naar de elektrode, maar slechts twaalf omdat een chip 16 signalen terugbrengt tot één. En 12 x 16 = 192. Twaalf draadjes passen binnen de omvang van een katheter, vertelt Rout, net de elektronica voor de signaalverwerking. Die miniaturisering biedt het perspectief van multikanaals signaalopnamen van het hart aan de binnenzijde via de lies, wat de methode inzetbaar zou maken voor verbetering van de diagnose.

Promovenda Sampi Rout werkt bij EWI aan de multiplexing van 16 signalen naar 1 om het aantal draden naar de elektrode te verminderen. (Foto: Jos Wassink)



 Trap er alsjeblieft niet in: biofotonentherapie met behulp van de Chiren.
Trap er alsjeblieft niet in: biofotonentherapie met behulp van de Chiren.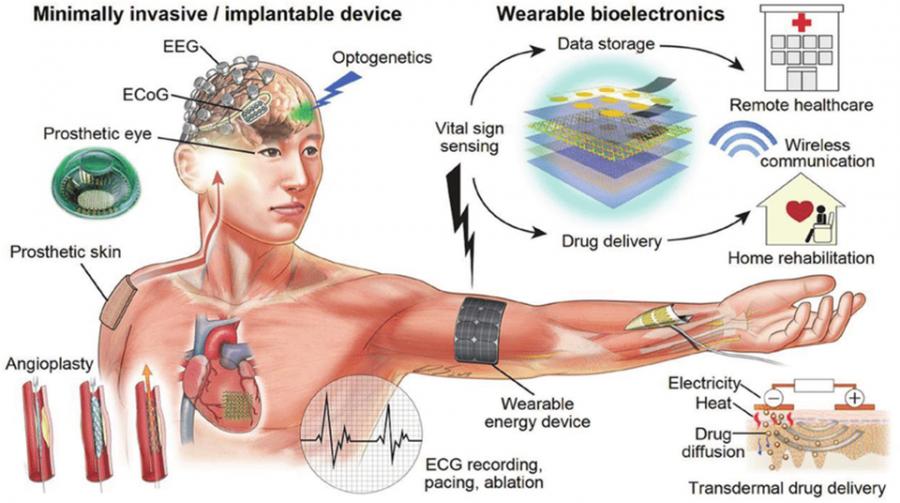 Are you in the final year of your BSc EE studies and interested in electronic medical devices? Then you may wish to consider continuing your studies in the MSc EE profile Biomedical Devices at Technische Universiteit Delft.
Biomedical devices are devices for medical diagnosis, monitoring, and treatment. They can be fixed, portable, wearable, implantable, and injectable. They are active and thus embed #electronics, computing, and software. Examples are: Magnetic Resonance Imaging (#MRI), Computed Tomography (CT), Positron Emission Tomography (#PET), #Ultrasound (US) imaging; Monitors for pulse oximetry, blood pressure, glucose, electrocardiography (#ECG), electro-encephalography (#EEG), electro-myography (EMG), electro-corticography (#ECoG), temperature, galvanic skin response, bio-impedance; Smart watches, smart patches, smart textiles, smart catheters, smart implants; Cardiac assist devices, cardiac pacemakers, implantable cardiac defibrillators (ICD); Devices for transcranial magnetic stimulation (TMS), transcutaneous electrical nerve stimulation (TENS), focussed ultrasound stimulation (FUS); Neurostimulators, brain-machine interfaces, organs-on-chip devices, #bioelectronicmedicine, #electroceuticals.
The Biomedical Devices profile has three focus areas = sub-profiles: 1. Biosensors, BioMEMS and Microsystem Integration (BioSemi), part of the EE track Microelectronics; 2. Biomedical Circuits and Systems (BioCAS), part of the EE track Microelectronics; 3. Biomedical Signal Processing (BioSP), part of the EE track Signals and SystemsFor registration, see:
Are you in the final year of your BSc EE studies and interested in electronic medical devices? Then you may wish to consider continuing your studies in the MSc EE profile Biomedical Devices at Technische Universiteit Delft.
Biomedical devices are devices for medical diagnosis, monitoring, and treatment. They can be fixed, portable, wearable, implantable, and injectable. They are active and thus embed #electronics, computing, and software. Examples are: Magnetic Resonance Imaging (#MRI), Computed Tomography (CT), Positron Emission Tomography (#PET), #Ultrasound (US) imaging; Monitors for pulse oximetry, blood pressure, glucose, electrocardiography (#ECG), electro-encephalography (#EEG), electro-myography (EMG), electro-corticography (#ECoG), temperature, galvanic skin response, bio-impedance; Smart watches, smart patches, smart textiles, smart catheters, smart implants; Cardiac assist devices, cardiac pacemakers, implantable cardiac defibrillators (ICD); Devices for transcranial magnetic stimulation (TMS), transcutaneous electrical nerve stimulation (TENS), focussed ultrasound stimulation (FUS); Neurostimulators, brain-machine interfaces, organs-on-chip devices, #bioelectronicmedicine, #electroceuticals.
The Biomedical Devices profile has three focus areas = sub-profiles: 1. Biosensors, BioMEMS and Microsystem Integration (BioSemi), part of the EE track Microelectronics; 2. Biomedical Circuits and Systems (BioCAS), part of the EE track Microelectronics; 3. Biomedical Signal Processing (BioSP), part of the EE track Signals and SystemsFor registration, see: 

 Tomas van Dijk @tomasvd
Redacteur
For questions/comments, email me at:
Tomas van Dijk @tomasvd
Redacteur
For questions/comments, email me at: 

